CASE REPORT
- Guillermo Careaga-Reyna MD 1
Medical Attention Unit, Mexican Institute of Social Security. Mexico.
High Specialty Medical Unit, General Hospital "Dr. Gaudencio Gonzalez Garza" CMN "La Raza", Mexican Institute of Social Security. Mexico.
*Corresponding Author: Guillermo Careaga-Reyna MD
Citation: Guillermo Careaga-Reyna MD (2024) *, Coronary intervention and ascending aortic dissection 1(1). Journal of Cardiovascular Investigations and Insights (JCII) DOI: https://doi.org/10.64347/3066-2613/JCII.001
Copyright: © (2024) Guillermo Careaga-Reyna MD *, this is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: February 13, 2024 | Accepted: March 09, 2024 | Published: March 26, 2024
Abstract
Introduction: aortic dissection associated with coronary interventions is rare.
Case presentation: This is a 33-year-old female patient with acute coronary syndrome who presented an aortic dissection associated to percutaneous coronary intervention and was treated with primary closure. Its evolution is satisfactory one year after the event.
Conclusion: Aortic dissection associated with coronary intervention is rare but may require surgical treatment that should be performed promptly.
Keywords: coronary intervention, aortic dissection, ischemic heart disease, right coronary artery, aorto-coronary dissection.
Introduction
Aortic dissection is a serious and deadly complication. It requires early detection and treatment [1,2].
It can be caused by atherosclerosis, high blood pressure, connective tissue disease or iatrogenic diseases, among other etiologies [1,3].
The association between aortic dissection and coronary intervention ranges between 0.02 and 0.04%, but in cases of urgent procedures for acute coronary syndrome it can reach 0.19% [2], and can be attributed to the mechanical trauma of the procedure, associated with the characteristics of the vascular wall, atheromatous plaque, among others [1,3]. Once diagnosed, treatment ranges from surveillance to the need for complex surgery of the aortic root with a higher risk of complications and mortality, determined by the clinical condition of the patient and the magnitude of the dissection according to the classification proposed by Dunning that establishes three types of dissection: type I that involves only the coronary vessels, type II where the dissection extends <40>40 mm dissection of the aorta. Type III dissection is where surgical treatment is recommended [1,4]. We present a case of aortic dissection associated with percutaneous coronary intervention to treat acute coronary syndrome.
Clinical Case:
The patient is a 33-year-old female, with no significant history, who presents deterioration of consciousness, so she was transferred to the medical care unit, where an acute coronary syndrome (ACS) was diagnosed, and in the hemodynamics room a right coronary artery obstruction was documented, which is resolved by placement of a medicated stent. An aortic dissection adjacent to the right coronary ostium not amenable to endovascular therapy was also observed [fig 1].

Fig 1. Angio tomography showing the type III aortic dissection.
Conservative management was decided. However, in her follow-up, an imaging study was performed that documented the presence of Dunning type III aortic dissection at the origin of the right coronary artery and in view of the lack of response to conservative treatment, surgical treatment was proposed, which was performed on February 21, 2023, via median sternotomy, under balanced general anesthesia with extracorporeal circulatory support, myocardial protection with HTK solution 30 cc/kg body weight, single dose. The repair consisted of primary closure of the origin of the dissection, near to right coronary artery ostium with two 6-0 polypropylene "U" stitches and a biopsy of the aortic wall was obtained. The procedure was performed without complications and the patient progressed satisfactorily. The follow-up study carried out on July 6, 2023, shows no evidence of remaining dissection [fig 2], and the patient is currently asymptomatic, performing her daily activities, only with treatment with antiplatelet agents. The result of the biopsy showed an aortic wall without pathological alterations.
Discusion:
Although underreported, the association between percutaneous coronary intervention and aortic dissection is low, but its diagnosis and care are very important, as it may require immediate surgical treatment [1-3].
In this case, it is striking that the infarction occurred in a young woman, although the fact that the affected vessel was the right coronary artery and the coronary intervention coincided with the dissection has already been described. It has been reported that the frequency of aortic dissection increases in emergency catheterization [2], and this fact is observed in up to 85% of cases, when the affected vessel is the right coronary artery due to its anatomical conditions [1,5], as occurred in our patient. When the dissection is small, it is usually left only with surveillance. In other cases, urgent pericardiocentesis or surgery may be required because the patient's life is at risk [2,4,5]. In this case, the patient underwent surgery with a type III Dunning dissection and in the face of a normal aortic wall, we decided on primary closure of the dissection, which was an effective and lower-risk procedure. During the follow-up, the favorable outcome of the study was verified.
Patients who are treated with percutaneous coronary intervention receive antiplatelet drugs and even anticoagulants, and in the event of a dissection, they would delay or prevent the formation of thrombus within the dissection, which, associated with the size, establishes the need to opt for surgical closure or replacement of the affected segment with a synthetic graft [1,2,5].
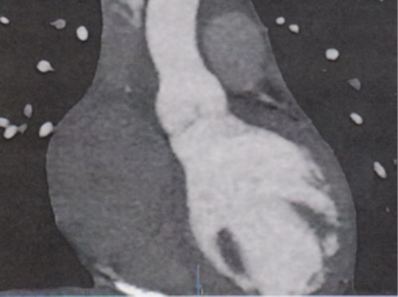
Fig 2. Posoperative Angio tomography without evidence of aortic dissection.
Conclusion:
Aortic dissection associated with percutaneous coronary intervention requires timely diagnosis and treatment to avoid complications and even death of the patient.
Funding:
This work was not funded.
Conflict Of Interest:
The authors declare that they have no conflicts of interest.
References
-
Yu C, He F, Chen H, Hong J, Qian X. Iatrogenic dissection of the right coronary artery and the ascending aorta secondary to percutaneous coronary intervention: A case report. Heart Surg Forum 2020; 23 (3): E366-E369.
Publisher | Google Scholor -
Fiddler M, Avadhani SA, Marmur JD. Guide catheter-induced aortic dissection complicated by pericardial effusion with pulsus paradoxus: A case report of successful medical management. Case Reports in Medicine, vol. 2015, Article ID 480242, 6 pages, 2015.
Publisher | Google Scholor -
Shah P, Bajaj S, Shamoon F. Aortic dissection caused by percutaneous coronary intervention: 2 new case reports and detailed analysis of 86 previous cases. Tex Heart Inst J 2016; 43(1):52-60.
Publisher | Google Scholor -
Dunning DW, Kahn JK, Hawkins ET, O'Neill WW. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000 Dec; 51(4):387-393.
Publisher | Google Scholor -
Sanchez-Jimenez E, Levi Y, Roguin A. Iatrogenic aortocoronary dissection during right coronary artery procedures: A systematic review of the published literature. J Soc Cardiovasc Ang Interven 2022; 1 (6) doi: 10.1016/j,jscai.2022.100443.
Publisher | Google Scholor -
Donabedian, A. (1997). The quality of care. How can it be assessed? 1988. Archives of pathology & laboratory medicine, 121(11), 1145-1150.
Publisher | Google Scholor -
http://www.scielo.org.co/scielo.php?pid=S0123- 93922022000200113&script=sci_arttext/plugins/pdfjs- viewer- shortcode/pdfjs/web/viewer.php?file=%2Fsite%2Fwp - content%2Fuploads%2F2019%2F10%2Fattention- indicators-
--> -
vih.pdf&download=true&print=true&openfile=false
--> -
Conceptual DYA, DDELA, Biological S, HIV AL, VDE Transmission, HIV DEL. Ultimas Normas, Servicio de Salud Colombia [Internet]. Hypertension Care Guide. 2000. p. 1–34. Available from: http://www.saludcolombia.com/actual/htmlnormas/nthipe rtension.htm Arn E. Viroimmune response and emergence of resistance in HIV-infected women receiving combination antiretroviral regimens for the prevention of mother-to- child transmission in Malawi. 2018; 69(3):9- 10.
--> -
Lethu T. Prevalent pregnancy, biological sex, and virologic response to antiretroviral therapy. 2018; 60(5):1- 2.
Publisher | Google Scholor